Healthcare is one of the few sectors where rising usage is treated as failure. That framing is wrong.
People want to be healthy, and the demand for services that help them conveniently get and stay healthy is practically limitless. But healthcare service delivery has always been rate limited by the cost and availability of clinicians; even perfectly aligned financial incentives can’t fix that.
AI alleviates that constraint. The technology drastically expands our capacity to provide care and drives down its marginal cost. Activity that was previously deferred, avoided, or dropped entirely enters the system because the system can finally absorb work it was structurally unable to handle before.
The extension of this is that AI gives us the opportunity to consume dramatically more of something – token consumption specifically, and agentic care services more broadly – and this matters a lot, for the purpose of getting this giant system to reorient itself in a new way. Agents are a new kind of service provider in health care of which we can consume an effectively unlimited amount, at tiny cost and huge volume, which is the opening you need to really transform a system.
The surprising obstacle here is that this is culturally incompatible with how we talk about healthcare. There’s a cultural posture in our society that says “consuming more healthcare is bad.” This comes from an understandable place, but it’s an attitude that holds back the change we actually want, if we want to make everyone healthier. In other industries, we talk about “Jevons Paradox” as this miracle of elastic consumption that helps ecosystems reinvent themselves: healthcare needs this to happen too.
The key question is actually very simple: how do we price AI-based care for abundant consumption? If we get this right, healthcare gets a technological and economic tailwind that benefits everyone. So let’s get it right.
Price Is Never Just a Price
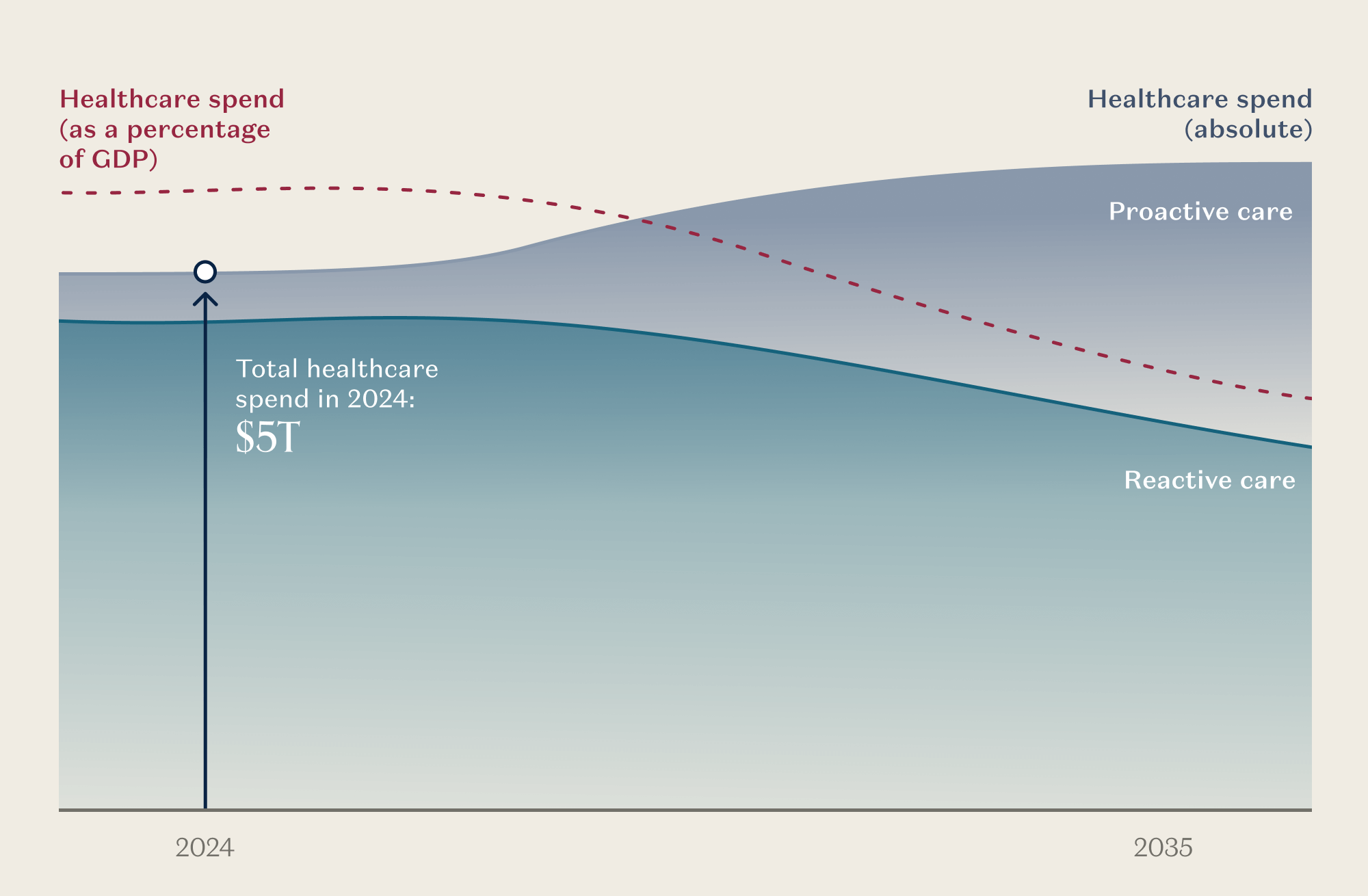
You may have heard of the “bitter lesson” in AI, which said that compute is the constraint on everything; to solve more problems, you just need more compute. Healthcare has always been that way, except instead of compute, it’s doctors. Since doctors and clinicians are expensive, and they’re rate-limited by their availability, the price of healthcare simplifies down to “more care = more expensive,” which makes the prospect of more consumption pretty scary. At a time when we already spend more on healthcare than anything else (~$5.3 trillion, or nearly 20% of our economy), how do we price this incoming influx of care capacity in a way that incentivizes innovation towards better health outcomes without breaking the bank?
Let’s start with the problem: why AI threatens to break the existing healthcare payment regime. Today, when a healthcare payor sets a reimbursement rate for a medical service, that rate implicitly assumes a certain volume to assess the overall budget for that service.
Price x Quantity = Total Medical Expense
Imagine if AI allows the quantity of a service to grow drastically, while holding price constant: total medical expense would increase unsustainably. The healthcare payor’s fear is straightforward:utilization explodes and costs go through the roof.
But the right question is not how to prevent that expansion. It’s “what do we get for it?” To answer that, we should consider the value of a healthier population.
The Value of Health
Today’s healthcare system is dominated by reactive care delivered after something has gone wrong, plus the administrative machinery required to ration access. This has drastic implications.
Imagine Jack, who begins life generally healthy. Sedentary desk job through his 20s and 30s, eating convenience food, no one nudging him otherwise. He develops hypertension by 40 – as nearly half of Americans do in adulthood. Heart attack in his 50s. A cascade of complications, expensive procedures, and comorbidities follows. Jack retires earlier than he planned. He is welcome to live as he chooses, of course. But the system never gave him a real shot at a different path.
Now consider Jill. Same starting point, but with abundant, proactive medical care – AI-enabled coaching, continuous monitoring, early intervention. Her conversations with her doctor feel personalized to her, and her care recommendations draw on the collective intelligence of the global medical community, not only the knowledge of her doctor down the road. She eats better, moves more, and sleeps well. Not because she’s more disciplined than Jack, but because the system is actually coded to help her stay healthy. She largely avoids the chronic disease cascade (hypertension, diabetes, obesity, and so forth) plaguing 75% of American adults today. Over the years she undergoes a couple of minor procedures, but her care team – human clinicians aided and extended by AI agents – checks in frequently after each one and guides her through recovery, helping her avoid rehospitalizations and downstream complications. Later in life, she goes on a couple of low-cost medications (for example, a GLP-1 agonist for her weight and a statin for her cholesterol), adheres to her care plan, enjoys her work, and retires on her own terms.
The value of Jill’s health to her is priceless. The value to society is enormous, and quantifiable across three dimensions:
- Reducing Avoidable Healthcare Expenditures. Half of all US healthcare expenditure in a given year is concentrated on roughly 5% of the population. A fifth of total spend is on just 1% – these are people suffering from the chronic disease epidemic, which is exactly where Jack ended up. AI that helps a patient stick to their medication regimen and avoid a hospitalization, or catches that cancer earlier at a screening and avoids costly treatment, generates outsized savings from a small number of patients. Medication adherence alone for chronic conditions like heart failure, hypertension, and diabetes generates a net savings of $1,300 – $7,800 per person per year while reducing hospital inpatient days by 1-6 days.
- Increasing economic productivity. When people are sick, they’re less productive, or drop out of the workforce entirely. The U.S. has roughly 160 million workers. If just 1%, about 1.6 million people and roughly half of a typical annual retirement cohort, work one additional year because they are healthy enough to do so, they generate approximately $260 billion in incremental GDP. If they work five additional years, retiring closer to 66, they create roughly $1.3 trillion in additional economic output.
- Increasing tax revenue. A healthier, longer-working population pays more into the system and draws less from it. In the scenario above, each additional year of work generates roughly $30 billion in federal, state, and payroll taxes from that cohort alone – while simultaneously deferring approximately $67 billion in Social Security and Medicare spending. Over five years, the combined fiscal impact exceeds $485 billion. And this effect repeats annually for each new cohort reaching retirement age (derived from IRS, SSA, and CMS data).
The value of keeping people healthy compounds across all three dimensions. The question is no longer whether we can afford to expand access to care. It’s whether we can afford not to.
Healthcare Business Models for Abundant Consumption
If the value of a healthier population is this clear, how do we build a pricing model that captures it?
As care capacity expands and friction to access care gets eliminated, consumption of care naturally increases, and the economic unit changes. Discrete visits lose prominence as the primary unit of care. Other industries have been through this transition before.
Telecom once priced voice and data by the minute because network capacity was scarce. As infrastructure improved, unlimited plans initially seemed risky, but usage increased without collapsing the system. Pricing shifted from entirely metering-based to primarily selling access, and total market value grew alongside consumption.
Music followed the same arc. iTunes sold songs one at a time. Spotify sold access instead. Listening exploded, consumer behavior reset, and track-by-track pricing faded. Consumer surplus expanded dramatically.
The general term for this is Jevons Paradox: as a service gets more affordable, we tend to consume dramatically more of it, and business models inevitably reorient from metering units to selling access. The business model shift is possible because there is something we’re consuming way more, which is what creates room for participants in the system to act opportunistically, and room for the system to adjust.
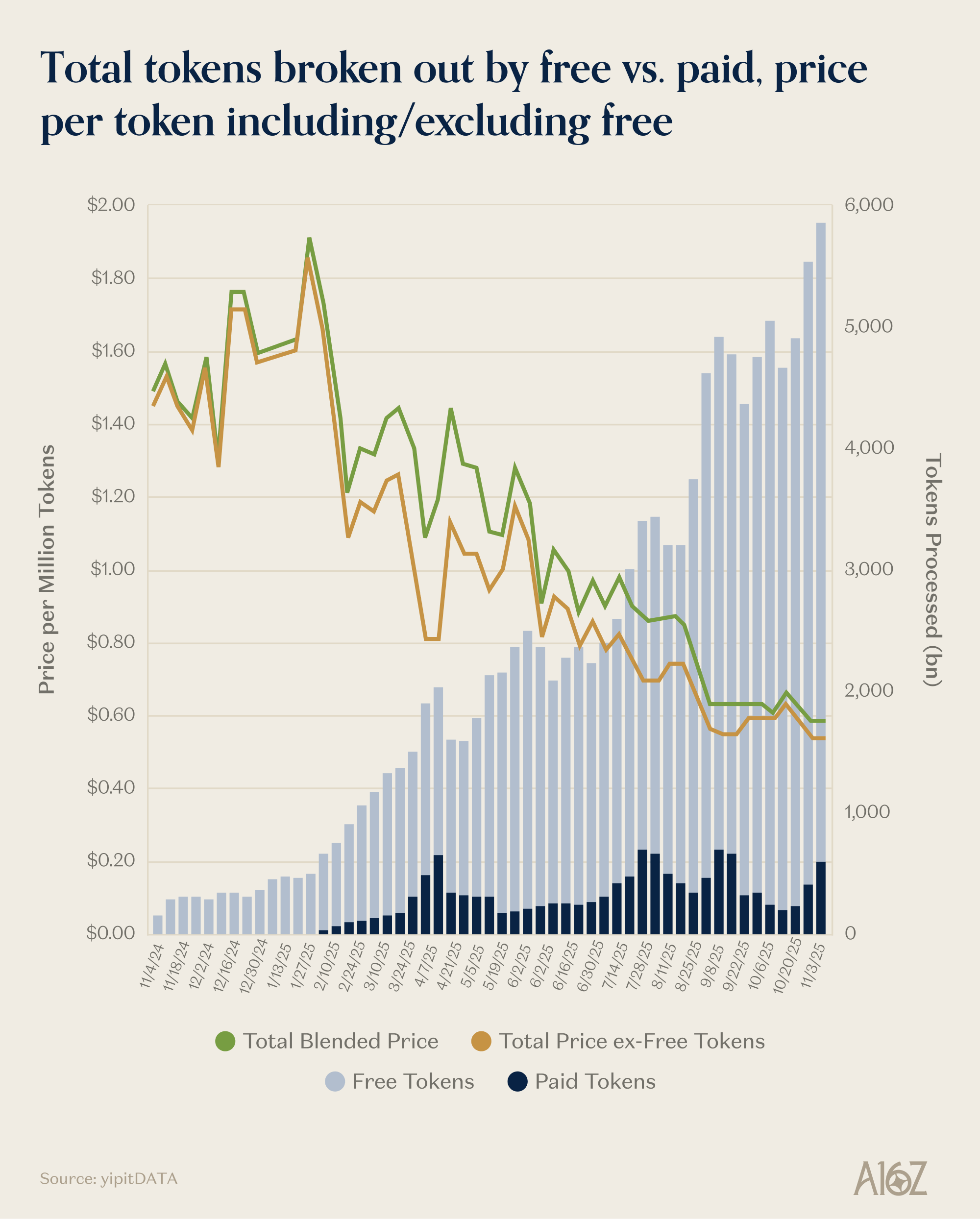
We love to see Jevons Paradox at a16z, and it’s everywhere you look in AI consumption
Healthcare is ripe for this shift. A significant portion of what gets metered today is information work – clinical evaluation, diagnostic reads, psychotherapy, triage. AI drives the marginal cost of that work toward zero. What stays expensive is physical: procedures, surgery, hands-on treatment. That separation is exactly what makes transformative pricing possible. Offer disruptively low cost or unlimited access to the information layer, and reserve fee-for-service for the interventions that actually consume scarce resources.
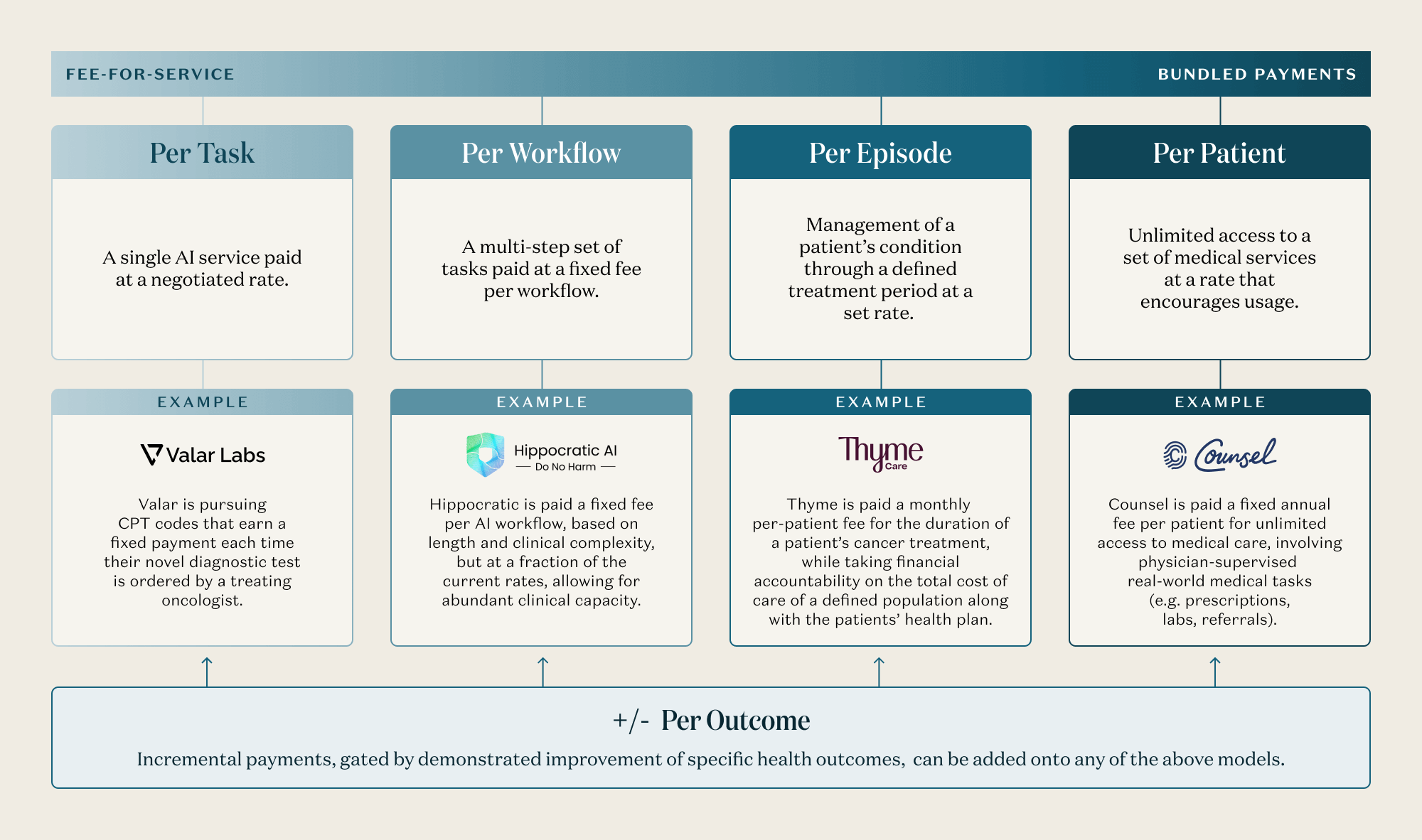
A growing number of companies are already operating along this spectrum, and AI-enabled care is being priced in at least four distinct models, running from task-based payments to unlimited access:
- Per Task: A single AI service paid at a negotiated rate.
- For example, Valar Labs has trained AI models that analyze cancer tissue pathology to predict which treatment will be most effective for a given patient, in a way that was never possible before with traditional molecular diagnostics. They are pursuing CPT codes that earn a fixed payment each time their novel diagnostic test is ordered by a treating oncologist.
- This could evolve into a transparent rate schedule for a range of AI diagnostic tasks (i.e. more AI tests, for more patients, with every kind of disease), conditioned on rigorous clinical validation data for each test and human-in-the-loop oversight. Each rate would be determined either by considering the existing reimbursement for the same task performed by a human clinician or the incremental value of that service, particularly when that service was not even possible before AI. While we envision dramatically increased consumption of many more AI diagnostic tests, the system would save billions in spend that would have been wasted on ineffective therapies for our patients.
- Per Workflow: A multi-step set of tasks paid at a fixed fee per workflow.
- For example, Hippocratic AI offers voice-based AI agents that call patients to handle sub-clinical tasks as an extension of their care team – scheduling wellness visits, answering intake questions, identifying care gaps, and more. They are paid a fixed fee, per workflow. Capacity can be spun up and down on demand, based on real demand, with a level of flexibility not possible with a human labor force.
- One could imagine a broader reimbursement schedule for AI workflows at fixed rates, with requirements that licensed clinicians retain final decision authority where appropriate – much like how services performed by a physician’s assistant under physician supervision are reimbursed today.
- Per Episode: Management of a patient’s condition through a defined treatment period at a set rate.
- For example, Thyme Care provides care navigation and clinical support to cancer patients. To deliver high-attention care around the clock with a sustainable cost structure, Thyme’s care team is augmented by AI tools that help them proactively predict issues, manage a complex network of in-person care providers, and triage patient concerns within minutes vs days. They are paid a monthly per-patient fee for the duration of a patient’s cancer treatment, while taking financial accountability on the total cost of care of a defined population along with the patients’ health plan.
- We could expand on this model by explicitly designating AI vendors as eligible “episode care managers,” authorizing multi-year, risk-bearing contracts for the management of a patient condition, contingent upon strong clinical validation and safety oversight.
- Per Patient: Unlimited access to a defined set of medical services, with “all you can eat” pricing that encourages the patient to utilize the service freely.
- For example, Counsel Health is a physician-supervised medical AI service that gives patients unlimited access to medical triage, medical advice, and clinical care. Patients interact with a personalized medical AI for the bulk of their needs, while Counsel physicians can authorize gated medical tasks, such as writing prescriptions, ordering diagnostics, and referring to specialists. Counsel is paid a fixed annual fee per patient.
- Additionally, payors could create reimbursement codes for subscriptions to a broad array of medical AI services that enable unlimited utilization of that service, paired with safeguards and clinical validation requirements to ensure patient safety.
Implicit in all of these pricing models is an additional tailwind: AI tools that automate administrative tasks, such as clinical documentation, scheduling, and intake, as Ambience and Tennr do for example, are helping clinicians work faster and more intelligently, expanding their capacity to care for more patients and creating the efficiency gains that make new pricing structures viable. Furthermore, any of these models can be paired with a “Per Outcome” overlay, in which some portion of fees are at risk, tethered to specific clinical measures. One implementation of this is CMMI’s Advancing Chronic Care with Effective, Scalable Solutions Model (ACCESS), which is a mix of Per Episode and Per Outcome payment models.
The Mix Shift That Matters
The natural objection to all of this: we already spend too much on healthcare, why would we want total consumption to go up?
Because the problem has never been the amount – it’s the allocation. We spend enormous amounts treating diseases that could have been caught earlier, managing chronic conditions that escalated because no one was watching, and administering a bureaucracy designed to ration access to a system that couldn’t handle more volume. We spend too much on the wrong things, too late.
As AI shifts our spend from reactive to proactive, we should be thinking first and foremost about what will improve health outcomes, and then about what we can be consuming more – daily or monthly, rather than annually – as AI changes the economics of care delivery. When more consumption saves money and makes us healthier, let’s increase consumption tenfold! What we want to see is the mix of healthcare spending shift away from costly, reactive care and towards proactive, continual service delivery.
So What Is Infinite Healthcare Worth?
More than we spend today, and more than current frameworks can recognize.
When capacity stops being the binding constraint, the question changes. It’s no longer about how to ration access to a fixed supply of clinician time. It’s about how much health a system can produce when access is continuous, affordable, and abundant, and when supply is infinitely intelligent, exceeding human reasoning capacity.
Infinite healthcare is worth more because it makes whole categories of care practical at scale that barely exist today: always-on monitoring, early signal detection, real-time guidance, and prevention – all of which need to occur before medical problems compound. It’s worth more because the downstream effects – a healthier workforce, fewer avoidable crises, a less burdened public system – multiply far beyond the healthcare sector itself.
The pricing models that win are the ones that recognize this. Not fee-for-service rates squeezed to reflect AI’s lower cost of delivery, but subscription and PMPM models that sell continuous access and align incentives with long-term health and economic growth. The companies that price for abundance rather than scarcity will capture the biggest prize: consumer behavior change, patient engagement, and true health outcomes lift. And the system that emerges – radically different in its composition of services – will deliver more health per dollar than anything we’ve built before.


